



Though self-harm is not a mental health disorder, it is often a symptom of other conditions, which makes understanding self-harm facts and statistics essential.
Self-harm involves a person damaging their body by cutting, burning, scratching or practicing any other behavior that results in pain or injury. Different motivators can encourage people toward self-harm, such as feeling overwhelmed or numb. Thoughself-harmis not a mental health disorder, it is a common symptom of many psychological conditions. Self-harm statistics and facts show the widespread trend of self-harm throughout the United States.
Article at a Glance:
- Self-harming behaviors include cutting, burning,andscratching oneself.
- The rates of self-harming behaviors are likely much higher than the statistics actually reported.
- Teens have the highest rates of self-harming behaviors.
- Self-harming behaviors are often co-occurring with eating disorders and substance abuse.
- Self-harm is not a mental health condition in itself, but treatment is available if self-harm is connected to drug and alcohol abuse.

Self-Injury Prevalence
Even though self-harm has been studied extensively for over a decade, findings are never entirely accurate because of the stigma and shame that still surrounds self-injury. The actual rates are likely quite higher than those currently reported.
One analysis of self-injuryacross more than 40 countries found that:
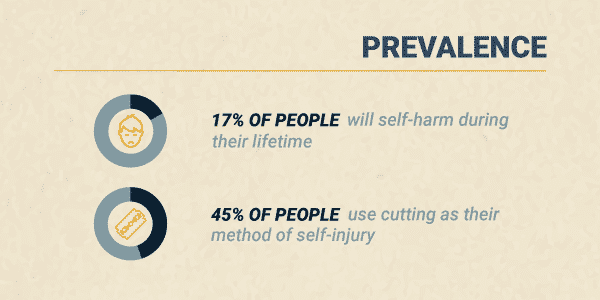
- About 17% of all people will self-harm during their lifetime
- The average age of the first incident of self-harm is 13
- 45% of people use cutting as their method of self-injury
- About 50% of people seek help for their self-harm but only from friends instead of professionals
Not only is self-harm prevalent, but rates are increasing. According toemergency room trends, there’s been a 50% increase in reported self-injury among young females since 2009.
Who Self-Harms?
While anyone can practice self-harm, rates tend to differ among certain populations:
- Adults. Aside from very young children, adults are the least likely group of people to follow through with self-injury. Only about5% of adultshave self-injured in their lifetime.
- Teens. Adolescents have the highest rate of self-injurious behaviors, with about17%admitting to self-injury at least once in their life.
- College Students. Studies find that about15%of college students report engaging in self-harm.
- Women vs. Men. While women are more likely to self-harm, males may represent at least35%of total self-injury cases. Men are more likely to underreport self-injury and have other people hurt them than women.
- Sexual Minorities.Gay and bisexual peopleare at a high risk of self-injury.Nearly halfof all bisexual females engage in self-injury.
Age of Onset
As mentioned, the average age of onset forself-injuryis 13. This age seems to align with new stressors and expectations at school and home as the child enters their teenage years. Age 13 represents a time of great physical, social and mental change and development. This time is also linked to the emergence ofmental health conditionslike anxiety and depression, which may further trigger a desire to self-harm.
Related Topic:How long does depression last?
Self-Harm Risk Factors
There is not just one factor that contributes to self-harm. Instead, there are a variety of biological and environmentalissues known to cause self-harm, including:
- Having friends or family members who self-injure
- Experiencing stressful life situations like traumatic events, family instability and sexual identity uncertainty
- Living in social isolation
- Mental health conditions, likedepression,anxietyandpersonality disorders
- Drug and alcohol use oraddiction
The more of these factors a person has, the higher their risk of self-harm.
Diagnosing Nonsuicidal Self-Injury Disorder (NSSID)
Nonsuicidal self-injury is not a diagnosable mental health condition: yet. Currently, the American Psychiatric Association (APA) lists nonsuicidal self-injury as one of the “Conditions for Further Study” in the most recent Diagnostic and Statistical Manual of Mental Disorders (DSM-5). This designation implies the group may include the condition in future versions of the text.
Nonsuicidal self-injury involves symptoms like:
- Engaging in self-harm on five or more days over the last year
- Self-injuring to find relief from an unwanted feeling, solve a relationship conflict or create a desired feeling
- Self-harm involves unwanted feeling like depression, anxiety or anger, an intense focus on completing the behavior and frequent thoughts of self-injury
Since self-injury is not currently an official mental health diagnosis, a medical or mental health professional will ask the person questions about the behavior and the purpose of the behavior to assess the situation.
Rates of Self-Harm and Co-Occurring Conditions
Self-harm often co-occurs with mental health disorders. Historically, self-harm was thought to be directly connected toborderline personality disorder. Now, it’s understood that the behavior can be associated with many conditions, like:
Onestudy foundthat of people who self-injure:
- 20% have personality disorders
- 13.5% have adjustment disorders
- 11% have mood disorders, like depression or bipolar disorder
Addition research shows that about55%of people who self-harm have eating disorders.
Although the conditions may overlap, nonsuicidal self-injury is often not linked to:
- Obsessive-compulsive disorder(OCD)
- Excoriation(skin-picking) disorder
- Trichotillomania(hair-pulling disorder)
Self-Harm and Suicide
Although an act of self-harm is different from a suicide attempt, there is a strong association between self-injury and suicide attempts. It seems that as incidents of self-harm increase, the likelihood of suicide attempts also increase.
People who engaged in 20 or more self-harm behaviors are about3.5 times more likely to attempt suicidecompared to those who have fewer self-injury actions.
Self-Harm Prognosis
Establishing a self-harm prognosis is based on:
- Frequency of self-harm
- Intensity of self-harm
- Duration of self-harm
- Presence of other mental health symptoms or conditions
- Available professional or social support
The APA reports in the DSM-5 that self-injury tends to peak by the time a person is 29, so the prognosis improves as age increases.
Statistics on Self-Harm Treatment
Since self-harm is not a mental health condition of its own, tracking treatment statistics is challenging. What experts do know is thattreatmentmust focus on the factors that trigger self-harm, as well as the self-harm itself.
For example, if yourself-harm is connected to substance use, getting help from The Recovery Village could reduce self-harm as you find recovery from alcohol and other drugs.Call todayto speak to a representative about available treatment options for self-harm and substance use disorders.
Comments